
CKD (chronic kidney disease) expected for 50% over age 30
 Chronic kidney disease (CKD) is rising steeply and projected to affect more than half of those aged 30 to 64 years in the coming twenty years according to a study just published in the American Journal of Kidney Diseases. The authors state:
Chronic kidney disease (CKD) is rising steeply and projected to affect more than half of those aged 30 to 64 years in the coming twenty years according to a study just published in the American Journal of Kidney Diseases. The authors state:
"Awareness of chronic kidney disease (CKD), defined by kidney damage or reduced glomerular filtration rate, remains low in the United States, and few estimates of its future burden exist...We used the CKD Health Policy Model to simulate the residual lifetime incidence of CKD and project the prevalence of CKD in 2020 and 2030. The simulation sample was based on nationally representative data from the 1999 to 2010 National Health and Nutrition Examination Surveys."
More than half of people aged 30 to 64 years likely to be affected
The authors' data showed that...
"For US adults aged 30 to 49, 50 to 64, and 65 years or older with no CKD at baseline, the residual lifetime incidences of CKD are 54%, 52%, and 42%, respectively. The prevalence of CKD in adults 30 years or older is projected to increase from 13.2% currently to 14.4% in 2020 and 16.7% in 2030."
Currently one in seven adults is affected by chronic kidney disease. The public health consequences are enormous. The authors conclude:
"For an individual, lifetime risk of CKD is high, with more than half the US adults aged 30 to 64 years likely to develop CKD. Knowing the lifetime incidence of CKD may raise individuals’ awareness and encourage them to take steps to prevent CKD."
Prevention: Metabolic syndrome and chronic kidney disease
 Components of metabolic syndrome (MetS) including insulin resistance, hypertension, dyslipidemia and inflammation are particularly rough on the kidneys. A review published in Current Opinion in Nephrology and Hypertension highlights the connection:
Components of metabolic syndrome (MetS) including insulin resistance, hypertension, dyslipidemia and inflammation are particularly rough on the kidneys. A review published in Current Opinion in Nephrology and Hypertension highlights the connection:
"The association of the metabolic syndrome (MetS) with cardiovascular risk, mortality, type 2 diabetes mellitus, stroke, nonfatty liver disease and gout is well known. However, the association of the MetS with chronic kidney disease (CKD) is now emerging...Studies show that patients with MetS have a 2.5-fold higher risk of developing CKD. The risk of microalbuminuria is also increased two-fold in the MetS. Renal dysfunction becomes apparent long before the appearance of hypertension or diabetes in MetS. Compared with healthy controls, patients with MetS have increased microvascular disease-tubular atrophy, interstitial fibrosis, arterial sclerosis and global and segmental sclerosis."
Clinicians should especially note that metabolic syndrome is contributing to chronic kidney disease well before it evolves into diabetes and the development of hypertension. Regarding potential mechanisms:
"Studies suggest that the renal fibrosis seen in MetS might be caused by a constellation of insulin resistance, hypertension, dyslipidemias and inflammation, and result in a heightened expression of adipocytokines, angiotensin and inflammatory cytokines such as interleukin-6 and tumour necrosis factor-alpha."
 The author of a paper published in the World Journal of Nephrology states:
The author of a paper published in the World Journal of Nephrology states:
"Despite the ambiguous definition of MetS, it has been clearly associated with chronic kidney disease markers including reduced glomerular filtration rate, proteinuria and/or microalbuminuria, and histopathological markers such as tubular atrophy and interstitial fibrosis. However, the etiological role of MetS in chronic kidney disease (CKD) is less clear. The relationship between MetS and CKD is complex and bidirectional, and so is best understood when CKD is viewed as a common progressive illness along the course of which MetS, another common disease, may intervene and contribute. Possible mechanisms of renal injury include insulin resistance and oxidative stress, increased proinflammatory cytokine production, increased connective tissue growth and profibrotic factor production, increased microvascular injury, and renal ischemia."
 The authors of a study published in PLOS One on the relation between metabolic syndrome and chronic kidney disease in an adult Korean population came to the conclusion:
The authors of a study published in PLOS One on the relation between metabolic syndrome and chronic kidney disease in an adult Korean population came to the conclusion:
"The strength of association between MS [metabolic syndrome] and the development of CKD increase as the number of components increased from 1 to 5. In sub-analysis by men and women, MS and its each components were a significant determinant for CKD...MS and its individual components can predict the risk of prevalent CKD for men and women."
Moreover, they excluded patients with diabetes to more clearly isolate contribution of metabolic syndrome to CKD. Commenting on the link between metabolic syndrome and chronic kidney disease in the development of cardiovascular disease in a paper published in Cardiology Research and Practice the authors note:
Commenting on the link between metabolic syndrome and chronic kidney disease in the development of cardiovascular disease in a paper published in Cardiology Research and Practice the authors note:
"Microalbuminuria has been described as the earliest manifestation of MetS-associated kidney damage and diabetic nephropathy, and it is associated with insulin resistance independent of diabetes. MetS is often accompanied by increased plasma renin activity, angiotensinogen, angiotensin-converting enzyme activity, and angiotensin II (renin-angiotensin-aldosterone system) and with renal sympathetic activity. Hyperinsulinemia, insulin resistance, and increased plasma angiotensin II levels are potent activators of expression of transforming growth factor-β1, a fibrogenic cytokine that contributes to glomerular injury."
Insulin resistance, of course, spurs chronic inflammation:
"The hallmark of MetS is insulin resistance. Inflammatory mediators, including tumor necrosis factor (TNF)-α, have been shown to mediate insulin resistance. Adipokines, including TNF-α, IL-6, and resistin, are cytokines secreted by adipose tissue, and their plasma concentrations are elevated in patients with MetS, whereas their plasma adiponectin levels are reduced. These findings may contribute to insulin resistance, and insulin resistance promotes chronic inflammation."
Sugar versus salt in hypertension and chronic kidney disease
 A striking paper just published in the journal Open Heart (British Cardiovascular Society) identifying sugar as a worse culprit than salt for hypertension and cardiometabolic disease further links metabolic syndrome and chronic kidney disease. The authors note:
A striking paper just published in the journal Open Heart (British Cardiovascular Society) identifying sugar as a worse culprit than salt for hypertension and cardiometabolic disease further links metabolic syndrome and chronic kidney disease. The authors note:
"Cardiovascular disease is the leading cause of premature mortality in the developed world, and hypertension is its most important risk factor. Controlling hypertension is a major focus of public health initiatives, and dietary approaches have historically focused on sodium. While the potential benefits of sodium-reduction strategies are debatable, one fact about which there is little debate is that the predominant sources of sodium in the diet are industrially processed foods."
But processed foods are high in sugar as well as salt, and it may be unwise to aggressively change sodium consumption...
'Strategies to lower dietary sodium intake focus (implicitly if not explicitly) on reducing consumption of processed foods: the predominant sources of sodium in the diet...Nonetheless, the mean intake of sodium in Western populations is approximately 3.5–4 g/day. Five decades worth of data indicates that sodium intake has not changed from this level across diverse populations and eating habits, despite population-wide sodium-reduction efforts and changes in the food supply.Such stability in intake suggests tight physiologic control, which if indeed the case, could mean that lowering sodium levels in the food supply could have unintended consequences. Because processed foods are the principal source of dietary sodium, if these foods became less salty, there could be a compensatory increase in their consumption to obtain the sodium that physiology demands.
Highly refined carbohydrates, the fuel for metabolic syndrome, worse than salt
This includes fructose:
"Coincidentally, processed foods happen to be major sources of not just sodium but of highly refined carbohydrates: that is, various sugars, and the simple starches that give rise to them through digestion. Compelling evidence from basic science, population studies, and clinical trials implicates sugars, and particularly the monosaccharide fructose, as playing a major role in the development of hypertension. Moreover, evidence suggests that sugars in general, and fructose in particular, may contribute to overall cardiovascular risk through a variety of mechanisms. Lowering sodium levels in processed foods could lead to an increased consumption of starches and sugars and thereby increase in hypertension and overall cardiometabolic disease."
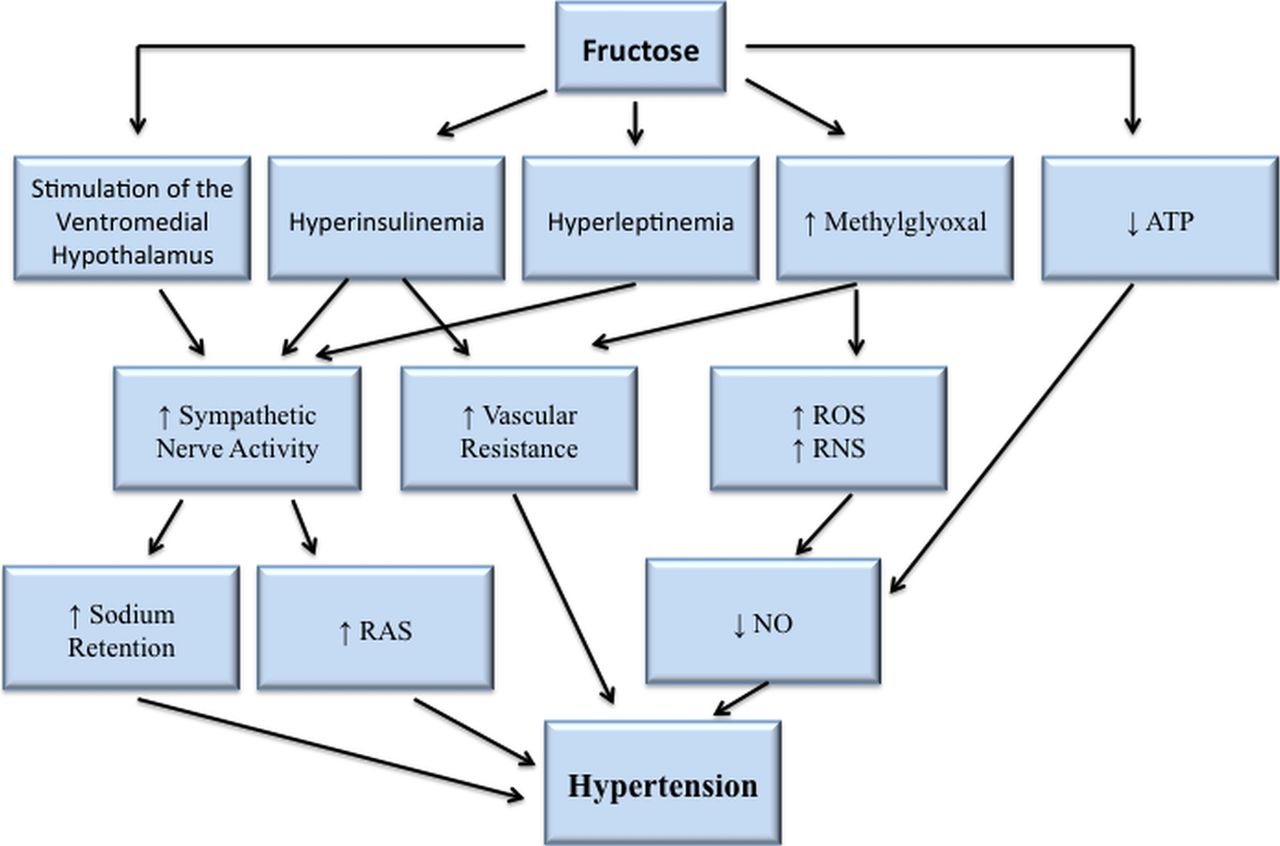
"Although high intakes of either fructose alone or sucrose may lead to insulin resistance, it is fructose that has been implicated as the sugar responsible for reducing sensitivity of adipose tissue to insulin.Insulin stimulates the SNS and hyperinsulinaemia may lead to hypertension, with the degree of insulin resistance in peripheral tissues directly correlated with hypertension severity. Reducing insulin resistance may lead to a reduction in blood pressure, and hyperinsulinaemia seems more related to fructose than glucose."
The authors make a distinction between fructose added to foods and that found naturally in whole fruit as stated in their conclusion:
"While naturally occurring sugars in the form of whole foods like fruit are of no concern, epidemiological and experimental evidence suggest that added sugars (particularly those engineered to be high in fructose) are a problem and should be targeted more explicitly in dietary guidelines to support cardiometabolic and general health...Evidence from epidemiological studies and experimental trials in animals and humans suggests that added sugars, particularly fructose, may increase blood pressure and blood pressure variability, increase heart rate and myocardial oxygen demand, and contribute to inflammation, insulin resistance and broader metabolic dysfunction. Thus, while there is no argument that recommendations to reduce consumption of processed foods are highly appropriate and advisable, the arguments in this review are that the benefits of such recommendations might have less to do with sodium—minimally related to blood pressure and perhaps even inversely related to cardiovascular risk—and more to do with highly-refined carbohydrates. It is time for guideline committees to shift focus away from salt and focus greater attention to the likely more-consequential food additive: sugar."
Quoted in Medscape Medical News, Richard Krasuski, MD, from the Cleveland Clinic in Ohio commented on the study:
""It is a little bit frightening that we have been focusing on salt for so long."...The conclusion that sugar represents a greater danger to the heart than salt, Dr Krasuski said, was an "eye opener." He acknowledged, though, that he should have anticipated it. He and other cardiologists have noticed that the recommendations to increasingly lower salt intake have not resulted in the expected positive cardiovascular outcomes."
Bottom line for chronic kidney disease
CKD incidence is rising steeply and projected to affect half the population aged 30 to 64. Key causal factors are metabolic syndrome with insulin resistance and hypertension. These are made worse by added sugars than by salt. Appropriate diet, objective determination of individual genetic and circumstantial needs for supplementation, regular exercise, not smoking, stress management and addressing sleep disordered breathing are common sense preventive and remedial measures.